How Antibodies Went From Bloodstream to Mainstream: Part 2
Currently, an array of antibodies is approved by the FDA for a range of therapeutic applications...
Twist Bioscience
December 12, 2017
5 min read
Micrograph of myeloma neoplasm from bone marrow biopsy.
Antibodies as Therapeutics – The Early Days
In 1908, Paul Ehrlich and Élie Metchnikoff won a Nobel Prize for their idea to develop a therapeutic compound that selectively targets a pathogen with a toxic agent. Work to leverage antibodies’ precise chemical selectivity for therapeutic purposes stalled after that initial conceptual breakthrough because the technology didn’t exist to produce specific antibodies at scale in a controlled manner.
Currently, an array of antibodies is approved by the FDA for a range of therapeutic applications, including cancer screening and treatment, autoimmune disorders, and infectious diseases. More hopeful antibody therapeutics populate the clinical pipeline every year. So how did we get here? Oddly enough, the profound positive impact of antibody engineering on modern medical practice wouldn’t have been possible without a type of incurable cancer known as a multiple myeloma.
Multiple myeloma is a cancer of the B Lymphocyte cells that produce antibodies. Unlike healthy white blood cells that can produce enough antibody variants to match the numerous harmful pathogens, multiple myeloma causes generation of an abnormal white blood cell population that produces huge amounts of a single type of antibody.
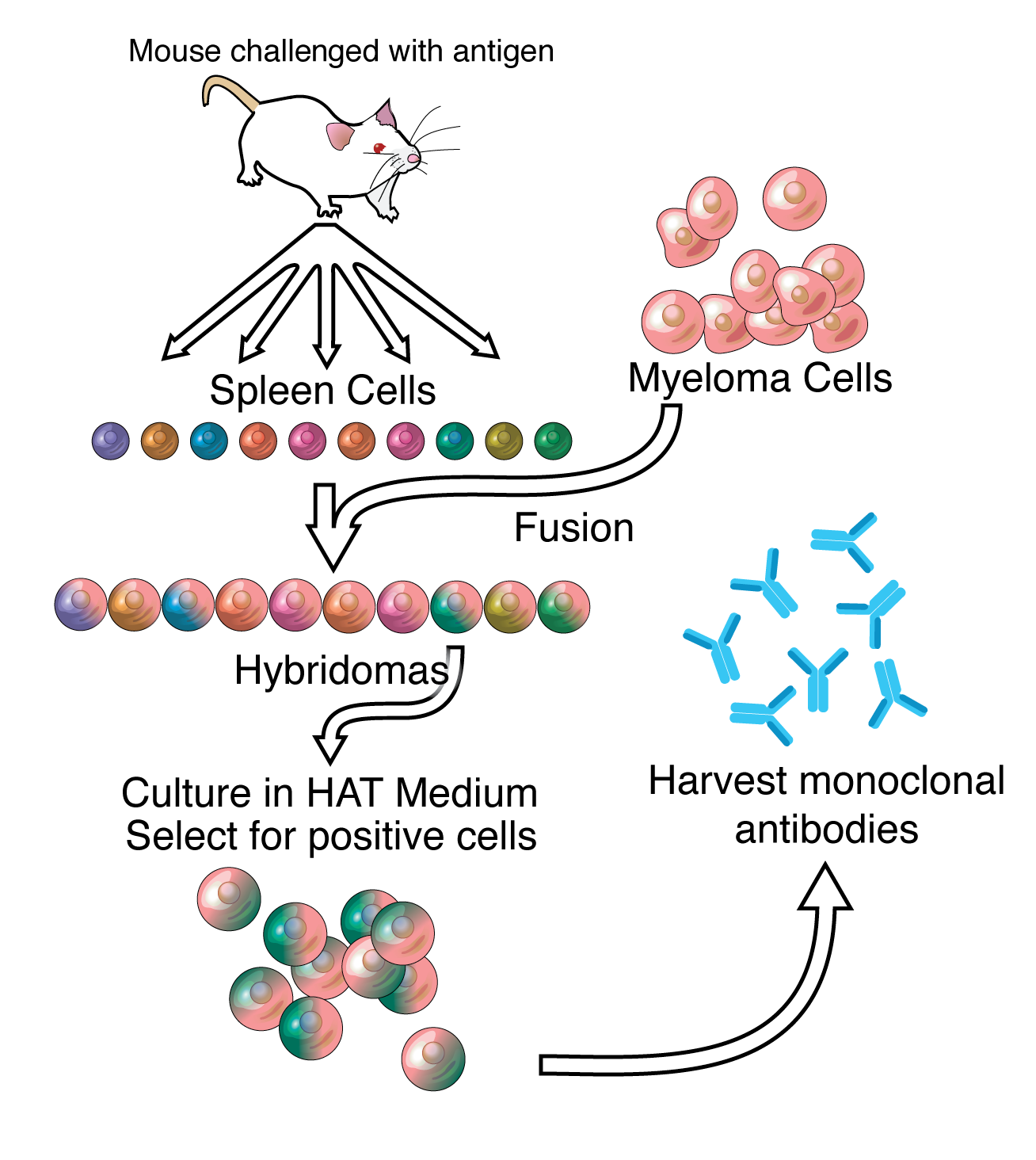
In 1975, researchers César Milstein and Georges Köhler realized that this peculiar quality of multiple myeloma cells presented a convenient solution to the problem of isolating and purifying a single antibody of interest out of the billions of different antibodies made naturally in an organism. They devised a method to fuse cultured mouse myeloma cells with mouse spleen cells that were immunized against a specific antigen. The result was a hybrid cell called a hybridoma.
Courtesy of https://upload.wikimedia.org/wikipedia/commons/9/9a/Monoclonals.png
After immunizing a mouse with an antigen of interest, spleen cells could be isolated and hybridized with a myeloma cell partner. This produces a hybridoma that generates an unlimited quantity of antibodies with selectivity for any antigen. Hybridomas can be cultured in the lab and frozen for later use, so once they are generated they can produce large amounts of antibodies forever.
Antibodies produced by Milstein and Köhler’s new method came to be known as monoclonal antibodies signifying that they derive from a single clonal cell population and all bind the same antigen. The invention of monoclonal antibodies and the subsequent standardization of their production laid the foundation for significant progression in the field of therapeutic antibody engineering. Once there was a reliable way to produce an unlimited supply of antibodies with selectivity for a specific antigen, researchers began focusing on clinical applications.
Antibodies binding to an antigen.
The first such applications of monoclonal antibodies were immuno-diagnostic. Hybridoma technology streamlined the production of antibodies with diagnostic properties by conjugating them with tagging enzymes or radioisotopes. These applications advanced basic research, improved diagnostic tools, and demonstrated the reliability and practicality of monoclonal antibodies.
However, the potential therapeutic applications of monoclonal antibodies, such as identifying clinically important antigen targets and selectively delivering therapeutic payloads, were still out of reach. Since the antibodies were derived from mouse cells, they were incompatible with human patients. Human lymphocytes would recognize the mouse proteins as foreign compounds and mount an immune response against the therapeutic agent.
It is of course risky and unethical to immunize human test subjects against dangerous antigens in order to produce human antibodies with the desired selectivity. This creates a need for a method to produce human antibodies in animal models. Serendipitously, the first step toward solving this puzzle was being developed almost simultaneously in the San Francisco Bay Area, in research that would bestow the Bay Area’s reputation as the birthplace of biotechnology.
In 1973 and 1974 Stanley Cohen at Stanford and Herbert Boyer at UCSF were laying the groundwork for the entire field of genetic engineering. Cohen and Boyer used restriction enzymes to fuse an animal gene with a bacterial plasmid. The desired gene product was amplified by allowing the bacteria with the recombinant DNA to reproduce naturally.
Using this recombinant DNA technique antibodies could be engineered with fewer non-human protein regions, enhancing the tolerability of therapeutic monoclonal antibodies in human patients. Although these new partially human antibodies were successfully implemented as therapeutics for several diseases, antibodies with any non-human regions could cause an immune response in a human patient which severely limits their efficacy.
Thus the challenge remained to produce monoclonal antibodies that were fully compatible with the human immune system. Producing an antibody with a high degree of affinity for a target antigen isn’t always as simple as instigating an immune response in a hybridoma progenitor cell, further complicating the implementation of therapeutic antibodies. That technique may work in theory and in basic research scenarios, but it’s difficult to bring to scale because of the intensive labor required.
Part 2 of a 3 part series. To learn more about antibodies, please read part 1 and part 3.